


The Innovation Killing Machine
While Create The Customer is usually topical, I’ll be taking opportunities to digress every once in a while and explore aspects of the healthcare system that are especially interesting or especially broken. I recently heard the story of a company that serves as a tangible example of how American healthcare’s broken incentive structure serves to limit and destroy technological innovation.
Our story begins with the invention of a force plate. A fitness equipment company’s overzealous R&D department turned up one day with a prototype for a wireless force plate sensor that would measure the muscle strength of the person pushing against it. They brought in some consultants to explore the commercialization potential in healthcare. Physical therapists, who regularly perform “manual muscle tests” to measure the strength of a patient’s muscles by resisting a push with their hand, were quickly identified as a customer. A new company, Kiio, was spun off to take advantage of this opportunity, and one of the consultants, Dave Grandin, was installed as CEO.
Grandin hit the ground running. They built a complete solution with the force plate to perform measurements and software that would digitally send instructions to the patient depending on the outcome of the test and the instructions of the physical therapist. They took this solution to physical and occupational therapists, and they loved it. Of course they loved it: it took the subjectivity out of a major and repeated test. It allowed them to practice better medicine because it took a strength test, graded based on feeling on a 1-5 scale, and provided objective mechanical accuracy of up to a hundredth of a pound. The software also enabled the physicians to see longitudinal data of how a patient was performing on these tests over time. It was clearly a better solution.
But it didn’t sell.
From the perspective of the physical therapist, the Kiio solution fell squarely on the cost side of the P&L. It represented an up-front expense that would improve quality, but do nothing to increase revenue. It would also mean training practice staff to use it properly. While they agreed it was vastly better from a clinical perspective, it was bad business.
The Terrible Triangle
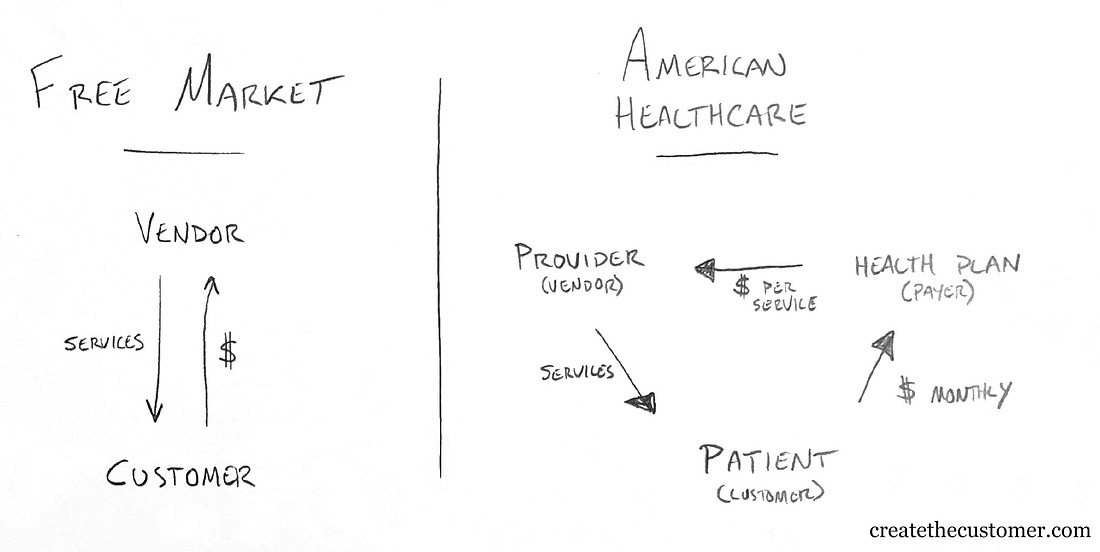
America typically operates as a free-market economy. For most things consumers are allowed to select a service or product from a slate of options and then exchange money for those services. If a product or service is bad, you choose a different one and the bad company either corrects their error or withers away. In aggregate (and not without exception) this works to weed out bad actors and reward companies that provide good value for the money.
In healthcare, you typically pay your health plan a fixed monthly premium, and they pay providers on your behalf. Because your health plan is a business trying to make a profit, they’re incentivized to reduce what they pay out to providers for services, allowing them to keep the balance of your fixed monthly payments as their operating capital and profit. Health plans achieve this by using their ability to direct patients as a negotiating tactic, meaning that if providers don’t agree to their proposed pricing they’ll be deemed “out-of-network” and thus receive no business from any of the patients in that health plan. In essence, health plans aggregate patient demand to drive down the cost of care.
Because of this system, providers are only incentivized to provide enough care (and often more than enough care) to bill your insurance company for the service. And because you must go to a provider who is “in-network,” you don’t have the agency to select a provider based on their merits. Providers thus have no reason to attempt to appeal to patients. If they are able to deliver care at the prices decreed by the health plans, they’ll be assured a steady stream of business.
The effects of this core triangle cascade outward through the system, turning what could be a straightforward value chain into a web of cost-shifting, concentrated power, and struggles for leverage.
The Innovation Killing Machine
When physical therapists evaluated the Kiio product they likely noted the clear clinical benefits, but bemoaned the fact it would bring them no new revenue. Health plans aren’t interested in providers running the most accurate tests; they just want the test to be inexpensive. It’s the same billing code for a muscle strength test whether the therapist uses his hand, an expensive force plate, or a banana. The therapists could have advertised their use of this advanced system to prospective patients, but it would likely barely move the revenue needle as most of their patients are simply directed to go there.
Had Kiio gone through expensive and time-consuming clinical trials to prove that there was a beneficial clinical outcome for a specific disease state when therapists used their force plate for muscle strength tests, there’s the chance they could use the aggregated demand of the provider community to force insurers to pay specifically for it. But that requires putting large amounts of capital at risk to pay for those trials, and Kiio found a better path.
With their newfound knowledge of the strange economics of healthcare, Kiio threw away the force plate and changed their offering to be simpler and laser focused on what the payer wants. They presented their software as a program primary care physicians could use to direct patients presenting with lower back pain to rehabilitative exercise rather than expensive back surgery. Suddenly the health plan benefited by paying a small amount to Kiio for each of these patients rather than paying a surgeon tens of thousands to operate. They appealed to the health plan’s key motivator: cost mitigation.
The dynamics of the healthcare system are such that an innovative product that improved overall quality and value was ultimately abandoned.
Kiio’s new product is generally a good thing. They’ve found a way to apply technology to reduce unnecessary surgeries, and did it in a way supported by the systemic incentive structure. This is largely the promise of digital health tools: chipping away at systemic inefficiency within the rules of the current system. They’re cool, they make little bits of the system work better, and they can make the companies that develop them a lot of money. But they ultimately do little to address the major systemic problems that kill actual innovation and subject Americans to a healthcare system with declining quality measures and increasing costs.
The real winners in the future of healthcare will be those who help push the system away from this terrible triangle of misaligned incentives and towards a value-based system, a system that rewards the entry of quality boosting technology.
Thanks for reading. If you enjoyed this post, consider sharing it with a friend!
This story was inspired by an interview with Kiio CEO Dave Grandin on Healthegy’s Breaking Health Podcast.