


#33 - Apple: Giving healthcare the iPod treatment
Dissecting Apple’s healthcare strategy, and more dispatches from the business of healthcare
Things That Happened
AC-Oh boy. The 2017 Medicare Shared Savings Program results are here, and things are looking good for ACOs. Farzad Mostashari, CEO of Aledade, went on a twitter rampage where he both analyzed the results, and shouted the good news from the proverbial rooftops:

6/ Lemme say that again....
ACOs saved Medicare over a Billion dollars in 2017.
Cheaper than FFS, cheaper than MA.
And they did it without cutting payments to doctors or narrow networks
And they did it with higher patient quality.
That's called delivering what was promised
What is the MSSP? Athenahealth has a high-level overview.
Also worth noting, Center for Medicare and Medicaid Innovation director Adam Boehler told MedPage Today this week that he thinks there are too few physicians in ACOs. Check out the full interview.
That’s one cool algorithm. Google has given control of their data center cooling systems over to a machine learning algorithm, and it’s reducing their overall energy usage by as much as 40%(!) When we talk about AI and ML in healthcare, the conversation inevitably focuses on clinical work and augmenting and replacing physicians. It’s important to consider how many ways ML can and will improve healthcare without entering the exam room. For example, Qventus is using ML to improve hospital operations.
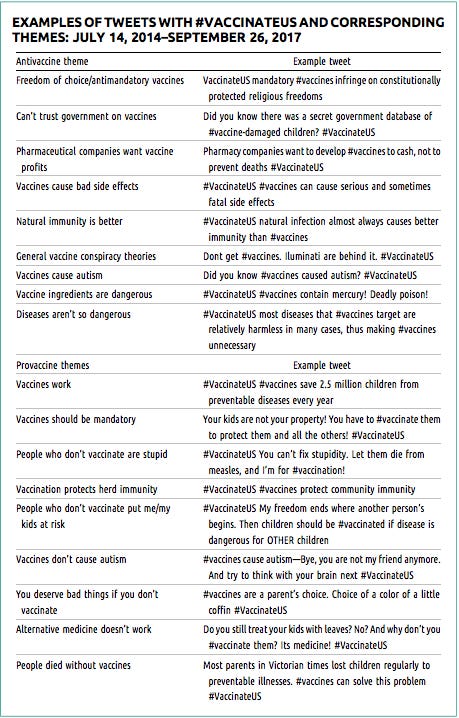
Robotic discourse. A group of researchers at George Washington University published a study showing that social media bots amplified the debate around vaccine usage. The trolls didn’t pick a side, but actually tweeted arguments on both sides (sometimes even from the same account) as a way of making the debate seem more vibrant than it actually was. The net effect: there’s yet another layer of complexity for laymen seeking health information on the internet, and this one is engineered to sway sentiments.
Things Worth Understanding
I’ve been tracking the various developments in Apple’s healthcare push, including their health records API and increased emphasis on wearables and health sensors. It seemed like a good time to consider the trillion-dollar company from Cupertino’s overall healthcare strategy, and what they’re bringing to the table.
When I first wrote about Apple’s health records API, I noted that we must consider all of Apple’s decisions from their overarching strategic goal: to sell more devices. Everything they do - all of their services and applications and sleek retail stores - exists to drive device sales. While in the past this has been computers, iPhones, iPads, and iPods, the company has recently added the HomePod speaker, AirPods, and the Apple Watch, with more wearable devices on the way.
Apple made their serious healthcare debut with the release of their health records API earlier this year. Going hospital by hospital, and health system by health system, Apple is creating an increasingly expansive list of relationships that enable the company to bring your electronic health records from your provider to your iPhone. And in true Apple fashion, they’ve made it exceedingly easy.
Apple has also been pushing forward on their wearable devices. Foremost has been the Apple Watch, which has started to transcend basic activity tracking into to more clinically relevant health information. While the watch itself can track basic beats per minute, when paired with the KardiaBand (pictured below) the device is able to take a clinical-grade EKG. In tandem with a Dexcom G5 continuous glucose monitor, the Apple Watch reports live glucose readings alongside data visualizations. These are just two examples.

To understand how Apple’s health records movement relates back to device sales, let’s examine the HomePod. Ben Thompson spent some time unpacking how the Apple Music service relates to selling these high-end home speakers:
Customer owns an iPhone
Customer subscribes to Apple Music because it is installed by default on their iPhone
As an Apple Music subscriber, customer only has one choice in smart speakers: HomePod (and to make the decision to spend more money palatable, Apple pushes sound quality), from which Apple makes a profit
In this view, Apple Music serves as a “bridge” to translate iPhone market share into smart speaker share; services is a means, not an end, which is exactly what we should expect from a company with Apple’s vertical business model.”
Adapting that same mode of analysis to health records and wearables:
Customer owns an iPhone
Customer syncs provider health records to iPhone
Customer now has the choice between using an Apple health wearable that will seamlessly carry all health data back to their complete health record on their iPhone (and their provider, in turn) or in using another company’s wearable.
In hosting your health records, and maintaining the link to the provider, Apple introduces an ease-of-use and holistic relevance to the use of health wearables that makes it almost foolish to purchase a non-Apple health device if you already own an iPhone.
Thus Apple will succeed in selling additional devices to existing iPhone customers, and will even go so far as to create a strong point of differentiation between iPhone and Android for those for whom health monitoring is a regular use case.
We can understand why Apple wants a part of the healthcare space, but what will Apple bring in terms of added value? To answer that question, we’ll travel back to 2001 and the birth of Apple’s digital hub strategy.
The conceit at the center of Apple’s hub strategy is that by connecting devices, software, and services together, you enhance the value of all of them. When Steve Jobs first laid out this hub strategy on stage in 2001, he gave the example of the camcorder. It works just fine on its own to record footage, but is ten times more valuable when paired with the iMovie software running on a Mac. The combination of the two allowed users to turn raw footage into finished pieces that could be shared.
The crux of the digital hub strategy was that it created and linked all the pieces required to reap maximum value from the device. Apple wanted you to buy an iPod, which was revolutionary in its own right, but recognized that without giving you the software to gather and manage a digital music collection, the iPod was far from useful. iTunes was just as critical to the success of the iPod as the iPod itself.
With the iPhone, the phone itself consumed the entirety of the hub. The magic happened when this platform was opened to developers. With the same standard peripheral devices - camera, microphone, speaker, accelerometer - all packed into the iPhone, developers were free to create every kind of niche application for utilizing these peripherals. This started as photo and video editing and sharing, and is now becoming augmented reality.
With the addition of advanced health wearables and sensors to the Apple ecosystem, that same magic is likely to happen. And it could solve the biggest problem with health wearables.
Daisuke Wakabayashi writing about the Kardiaband in the New York Times:
A flood of information, albeit potentially useful, may overwhelm doctors instead of assisting them. Initially, KardiaMobile patients sent their doctors an email each time they took an EKG reading. The flood of emails became confusing and raised questions about where the doctor should store that information. In response, AliveCor introduced a software platform for doctors that could populate the readings from patients and help detect early signs of atrial fibrillation.
Doctors don’t want, nor do they have the time, to pore over a patient’s longitudinal heart rate data. While it may be interesting that a patient has seen a 10% decline in average time spent sleeping over the past month, there’s no way for a doctor (or the patient) to notice this trend in the raw data from their sleep tracker. Health data from wearables is, to paraphrase Mr. Wakabayashi, a flood of information that’s potentially useful.
There’s immense opportunity for a middle layer of logic that can extract the relevant signal from the noise. As AliveCor discovered, a preponderance of data ultimately serves to hinder its utility. What’s needed is that middle software layer that tempers the flood, and extracts exactly what’s useful.
With their health records API, and the growing inclusion of gathered health data, Apple is laying the groundwork for a truly consumer focused health app store. This middle layer will make the data gathered by health sensors useful, contextual, and clinically relevant. It will allow developers to create thousands of applications like AliveCor’s EKG solution, except they can be targeted at every niche use-case that can can derive insight from the underlying data. What’s more, these applications can marry the data from various streams, extracting insight from a patient’s EKG compared with sleep tracking and step count.
Most importantly, using Apple’s health records API, the insights from these applications can be carried directly into an EHR system. Apple has created a continuum of health data from the sensor on the patient’s body into the clinical EHR, with opportunity for intermediate contextualization and analysis.
In short, Apple is positioned to do for health wearables what they did with the iPod. They’re creating not just the device, but the enabling ecosystem that makes the device more valuable and useful.
Things To Read
On the Health Affairs blog, Amol S. Navathe, Eric Shan, and Joshua M. Liao answer the question: What have we learned about bundling medical conditions? They argue that while medical condition bundles haven’t shown the same savings as surgical bundles, there is still more work to be done in designing these bundles to better suit the more complex, ill-defined, and chronic nature of medical conditions.
“a neural net has many different and equally good ways of modeling the same data set,” writes Geoffrey Hinton in JAMA. Last week we heard from Optum’s AI chief, Sanji Fernando, on the ‘black box’ problem of deep learning, where clinicians can’t evaluate an AI’s decision by understanding the process through which it was made. In this piece, the legendary Hinton, who is considered ‘the godfather of deep learning,’ lays out how deep learning neural networks approach a problem, and why it might be infeasible to expect to be able to follow along.
“While Comcast continues to work with insurers, it has largely shunned them as a source of innovation,” Reed Abelson writes in The New York Times. Comcast, your least favorite company to deal with, has kept their healthcare spend on employee coverage largely flat over the past 5 years, and they did so while keeping a $250 deductible for their members. Their method: actively recruit, invest in, and direct employees to use a patchwork of services that help them better manage their health and healthcare usage. It’s an n of 1 situation, but stands as another example in the heaping pile of evidence that old-line insurers aren’t going to be the source of healthcare business innovation. Let’s hope Comcast decides to start being as nice to their customers as they are to their employees.
“There is a framework I’ve/we’ve used over the years to think about where to invest and where not to invest that I call ‘atoms vs bits.’” Fred Wilson, co-founder of Union Square Ventures, explains this underlying investment thesis on his blog. Software - bits - is quicker to mature and reap value than innovations that deliver value through physical means - atoms. There’s nothing revolutionary here, but it’s an interesting heuristic for quickly appraising the near and long-term prospects of new ventures.
“Small data is not in style these days,” Dr. Isaac Kohane writes for WBUR. He argues there is a lack of emphasis on accuracy in data collection these days, which is especially troubling given the growing role big data plays in our decision making. “… there's a disturbing gap between the theoretical use of these measurements and the accuracy with which those measurements are made.” As they say: garbage in, garbage out.
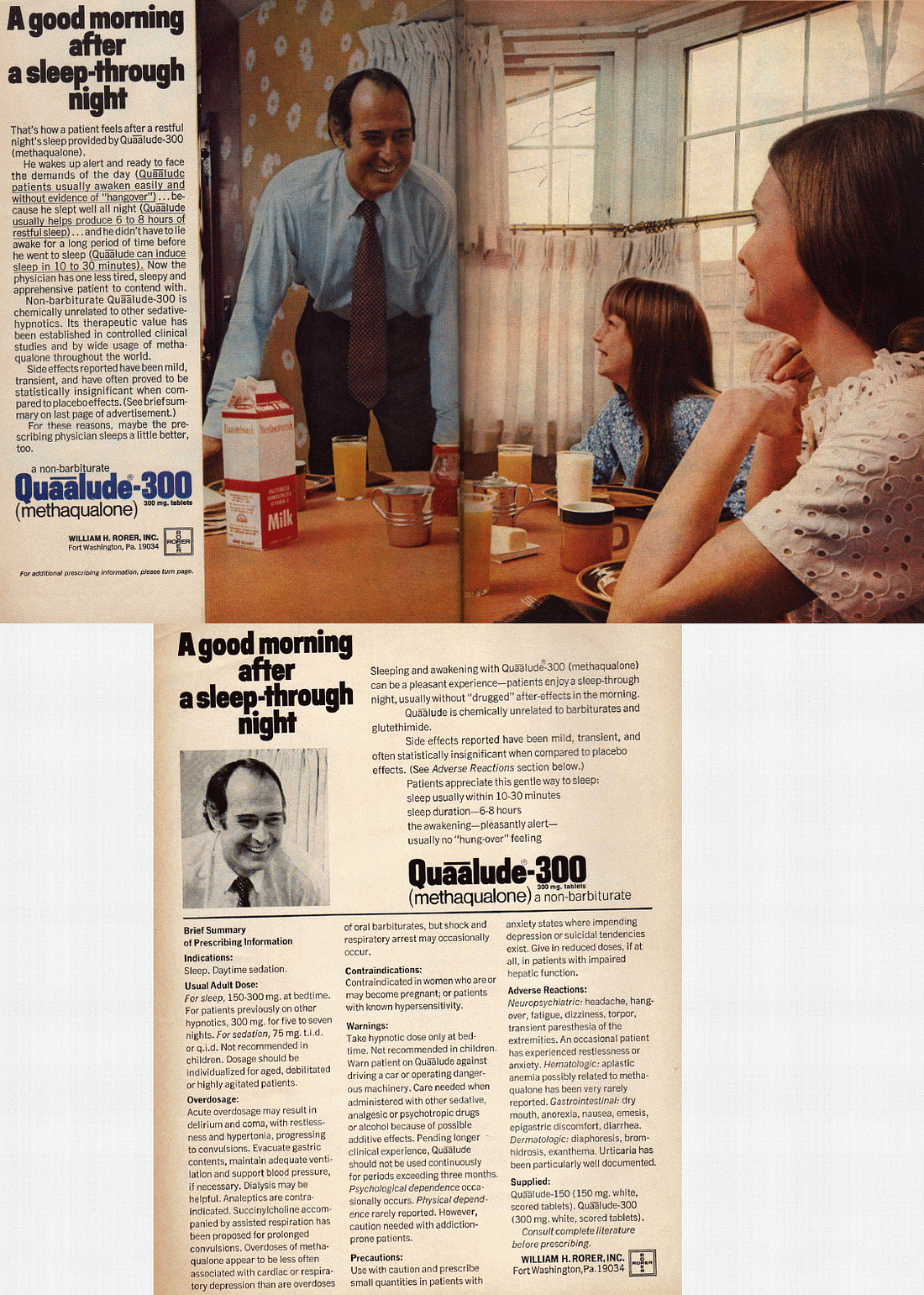
And here’s a list of 35 prescription drugs that were pulled from the market. Quaaludes included.
 Handout University
Handout University
It’s a holiday today, so you probably have a little more time than normal to delve into some light reading. What better time to get an update on quantum computing and networking?!
Unlike artificial intelligence, quantum computing is still fairly futuristic as it hasn’t been practically deployed to any real extent. That said, it’s still worth understanding what it is and the promise it holds for the future. You don’t want to be the only one at your labor day BBQ who hasn’t considered the processing and networking applications of quantum entanglement.
The race is on to dominate quantum computing from The Economist
The quantum internet has arrived (and it hasn’t) from Nature
Things I Listened To
The air was mercifully warm and crisp in Vermont this week, which makes for perfect admiring-the-sunset-weather. There’s no better soundtrack for summer evenings that Nick Drake’s Pink Moon. (spotify)
Enjoy your holiday,
- Isaac
Thanks for reading The Healthcare Handout, a weekly update on the business of healthcare from Isaac Krasny. You can find him at isaac@healthcarehandout.com, or on twitter @isaackrasny