


#29 - What We Should Talk About When We Talk About AI
How to cut through the hype and see what’s really going on in AI
Settle in and get your clicking finger ready. This one’s packed with good stuff.
Things That Happened
Walgreens launched an app - both on the web and mobile - to help people find providers. Pretty much any kind of provider, according to Walgreens VP Giovanni Monti: “…You can have access to house call doctors, urgent care, primary care, second opinions, labs. Some of these services are colocated in our store, others are at home, and others are online, so it’s multichannel in a way.” It’s curated to ensure only “highly regarded” providers are presented to users. It also includes Walgreens provider locations, naturally.
It’s an opening salvo from the retailer in an increasingly busy battlefield around controlling the flow of patients through consumer friendly apps. I wrote about K Health and their similar strategy a few weeks ago, and WebMD just acquired the consumer services division of Vitals. This division includes tools that help patients find and compare physicians.
Ultimately, the question is whether these digital tools can wrest control of patient flow from insurance companies and doctors. Stories below on how patients don’t really shop for care, and Walgreens’ larger strategy.
English Robot Doctor Heads East. Babylon Health, the UK company applying AI to primary care and insinuating they want to replace human doctors, has signed a deal with Prudential Asia for the use of their chatbot and health assessment technologies. Rather than using these tools primarily to help their existing members, Prudential plans instead to deploy them as marketing tools. Health insurance is optional in many markets, and thus offering a shiny digital tool may convince people to take a second look at getting a policy. While the use case is different than the population health model we usually consider for tools like this, the basic question is the same: can a digital tool get people more engaged in their health?
File under: “Things that are happening.” As The Economist notes, private equity firms have gotten back into the habit of investing in healthcare, indicating 2017 was the biggest year by deal value since 2007. Private equity has a fairly standard playbook: buy something, make it more efficient and profitable, then sell it for more than you paid.
The problem for healthcare is that private equity will maximize revenue in the short term, meaning further stress on existing broken incentive systems. You could make an argument that short term thinking is one of American healthcare’s biggest problems, and one that will only be exacerbated by private equity’s renewed fondness for the industry.
Alexa may be a bad doctor, but she’s already making house calls. A report this week estimates that of the 50 million smart speakers in American homes, 70% are Amazon devices. As Amazon wants to compete in the aforementioned battleground of controlling patient flow through consumer friendly apps, this foothold of 35 million devices (a channel in which they have total control) will prove exceedingly valuable. MobiHealthNews just looked at 37 startups currently developing voice-based healthcare apps.
This is the same sort of market penetration and control that’s making it possible for Apple to do what they’re doing with health records. While many (many) companies have set their sights on being the Amazon of healthcare, perhaps Amazon is going to be the Amazon of healthcare.
Things Worth Understanding
“The discourse is unhinged,” according to Oscar Schwartz in The Guardian. Going back to the days of ENIAC, one of the first modern computers to exist, Schwartz spells out a cycle that repeats itself with new technologies. Inventors describe modest gains, which is then turned into speculative and overblown coverage by the media. When those grandiose speculations prove unfounded, there’s a backlash that effectively debunks the claims the innovator never made, and people grow skeptical of the new technology’s promise. All the while, in the background, technologies continue to actually improve.
An example from Schwartz’s piece :
While the “perceptron” could only be trained to recognize a limited range of patterns, the New York Times published an article claiming that the algorithm was an “electronic brain” that could “teach itself”, and would one day soon “be able to walk, talk, see, write, reproduce itself and be conscious of its own existence”.
This comes from 1958. We obviously don’t have those capabilities 60 years later, so it’s easy to see why people are skeptical of the hype. They probably should be.
I don’t want to lay blame entirely on the media. Social media is a prime target for overblown claims of technological innovation, and there are enough hucksters and salesman in technology circles trying to convince people we’re further along than we actually are.
It certainly doesn’t help the case for AI when technology fails publicly. Most recently it was Stat’s report that IBM Watson was recommending ‘unsafe and incorrect’ cancer treatments. The meat of the report was that Watson’s training was done on demonstration cases created by researchers and physicians, rather than on actual patient data.
Another shade of AI criticism has come in the form of unearthing companies that claim to be using AI, but really have human laborers behind the scenes. The MIT Technology Review published a brief saying “There isn’t always a computer program behind ‘AI’ services—sometimes it’s just plain old ‘I.’” Among the examples cited were a company that claimed to use computer vision to transcribe images of receipts for expense reports, when they were actually farming the work out to human transcriptionists.
Criticisms like these, however, miss the point. When it comes to evaluating artificial intelligence, we shouldn’t focus on process, but instead on value.
You could create a company that transcribed images of receipts using human transcriptionists, or you could create one that did the same using a computer vision algorithm. The benefit of the latter approach is scale: the algorithm can do the work infinitely faster and indefinitely without getting tired. And it’s a fixed cost. Assuming the quality of the transcriptions are comparable, the CV based service can be offered at a much lower cost. Often, recording the data of a controlled human process is the only way to automate it with AI.
Value, the intersection of cost and quality, is the key driver behind the adoption of artificial intelligence. IBM could have set up a service where oncologists send their patient files to a group of 100 highly-trained oncologists, who would then evaluate the files and arrive a suggested diagnosis and treatment. That, obviously, would cost quite a bit. The promise of AI is that you can replicate a cumbersome process in a set of algorithms that, once you’ve invested time and money in training them, have no variable cost.
Good AI delivers the quality expected from human labor, but at the cost of an AI solution. Thus it doesn’t matter what’s actually going on behind the curtain to arrive at the outcome. What matters is that the outcome is of equal or better quality than if a human had done it, and delivered at a more favorable price.
When evaluating an AI solution, focus on value, not process. It frankly doesn’t matter what data IBM used to train Watson. If they had produced a service that would reliably provide valuable treatment recommendations to physicians, nobody would ask or care how they had done it. Pharmaceuticals aren’t judged on the process by which they’re discovered, but instead on their safety and efficacy in treating disease.
Where are we in the cycle of AI acceptance? There have certainly been lofty claims and big questions. IBM has been touting their AI solutions for years (remember Watson’s turn on Jeopardy?). There seems to be a new article weekly about which jobs robots will take next. The Guardian asked just this week in a headline: “The robot will see you now: could computers take over medicine entirely?”
And then there’s the pushback: unmasking companies that aren’t as advanced in AI as they want you to think, and revealing that IBM’s solutions aren’t actually so good (or are just plain shitty.)
So the answer is an obvious one: AI is here to stay. If you look for the value being delivered, it’s there, and it’s real. There will be those overstating progress, and those calling them out on it. But there is quiet and steady progress occurring, and it is enabling new business models and models of care that otherwise couldn’t exist.
My favorite method for evaluating stories based on their headlines is Betteridge’s law: Any headline that ends in a question mark can be answered with the word no.
Things To Read
Want a refresher on all of Apple’s healthcare moves in the past decade? Ryan Black has you covered.
“…the identity of a patient’s orthopedist explains a lot more about where he or she got her M.R.I. than any other factor considered, including price and distance,” writes Austin Frakt in his piece in The New York Times about shopping for health care services. In the above example, Frakt cites a study in which researchers tracked non-emergent lower limb MRIs, an extremely “shoppable” procedure, and found that almost nobody actually shopped, even when they were on the hook for the cost. This aspect of consumerism in healthcare doesn’t seem to exist.
“Under North Carolina’s law, a medical provider must obtain a government permit (a ‘certificate of need’) if they want to offer certain new services or buy new equipment.” Dr. Gajendra Singh argues this creates monopolies that allow current MRI providers to charge high prices for scans, while he is barred from purchasing an MRI machine and providing scans at half the cost. While government control over supply certainly constrains marketplace forces on pricing, we can draw conclusions from Austin Frakt’s story above that half-priced scans probably wouldn’t do much to bring down the average price. While Dr. Singh’s story is frustrating, it doesn’t seem to hold the key to lowering healthcare prices. Dylan Scott writes about Dr. Singh’s lawsuit this week in Vox.
“While Amazon and Google get lots of positive PR and media attention as major healthcare industry disruptors, don’t forget about two big ‘W’s,’ Walgreens and Walmart, in the healthcare innovator mix,” Jane Sarasohn-Kahn wrote in a post on Health Populi. She further explores Walgreens Find Care Now app, discussed above, and Walmart’s various signals that they’re getting more serious about healthcare.
As Owen Tripp pointed out on a recent episode of the Tech Tonics podcast, there won’t just be one of these tech/retail companies that “wins” healthcare - there will be many.
If you’re looking for even more insight into Walmart’s plans in healthcare, Marcus Osborne, their VP of Health & Wellness Transformation, gives a pretty candid interview on the most recent episode of A Healthy Dose. The quick version: it’s healthcare services. Also did you know that, according to Osborne, Walmart does more health risk assessments every week than the entire US healthcare system? Seems like they could have an impact on the space.
A follow up from the story I included last week on Regeneron:

George and Len from $REGN didn't much like my recent profile of them. They think everyone in healthcare is focusing on the wrong things -- and they explain here. https://t.co/6ewGo3C6Vw
July 31, 2018Handout University
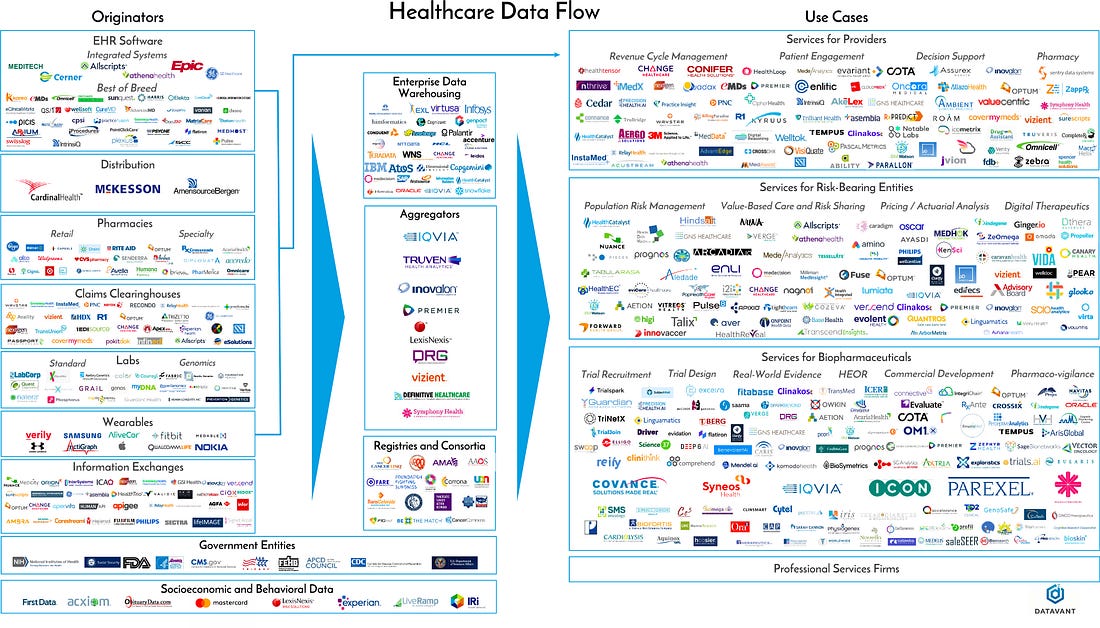
This article, from the team at Datavant, maps out the flow of healthcare data from the patient up. It also includes the expansive, and expansively cool, chart above. If you feel like you could know more about healthcare data, take a look.
One interesting takeaway: we must remember that most of the tools for gathering healthcare data are designed to meet the operational need of the purchasers. Your primary care doctor’s EHR is designed to track his patients and the details he cares about, while your oncologist’s EHR is designed to do the same, but according to her unique oncological workflow. Neither is geared towards data collection for retrospective studies or mass reporting. Remember this as you encounter critics decrying the sorry state of our healthcare data. We are still in the relatively early days of broad-based digital health tracking.
Things I Listened To
This week was very much all about Sylvan Esso in the listening department. Amelia’s voice, Nick’s beats. It just works. Both their self-titled breakout debut, and their appropriately titled follow up What Now are worth checking out.
Comments? Praise? Disagreements? Music recommendations? You can always email isaac@healthcarehandout.com or find me on twitter @isaackrasny
Stay healthy,
Isaac